
‘Torsade de pointes’ (‘twisting of the peaks’) is a form of polymorphic ventricular tachycardia. This most enigmatic and aesthetic of ECG findings was originally described in a patient presenting to Hôpital Lariboisieré, Paris, with episodes of syncope in February 1965.
A tachycardia in which rapid ventricular depolarization is maintained by a pathogenic mechanism located exclusively in the ventricular tissues. Electrical communication between ventricular and extra-ventricular cardiac tissues may occur in this arrhythmia but, by definition, such communication is not required to maintain the tachycardia.
Any tachycardia not satisfying the above criteria.
An elderly woman presented to ED/ER having experienced an episode of collapse. Her 12 lead ECG on admission showed sinus rhythm with prolongation of the QT interval (605 ms). She was stable at presentation and was placed on a cardiac monitor. An event recorded on her monitor approximately one hour post-admission is shown below.
The patient has developed a polymorphic ventricular tachycardia (VT).
‘Monomorphic’ VT (strip below): The morphology and axes of the ventricular deflections is constant in a given lead. The arrhythmia is broad complex with a regular occurrence of qrs complexes.

‘Polymorphic’ VT (strip below). The morphology and axes of the ventricular deflections varies in an individual lead with time. The arrhythmia is broad complex with an irregular occurrence of qrs complexes..

Torsade de pointes: the combination of polymorphic ventricular tachycardia and prolongation of the QT interval on the ECG.
The paroxysm of tachycardia in the case study presented here beautifully illustrates the classical ECG features of torsade de pointes (‘twisting of the peaks’) as described in Dessertenne’s original paper (1).
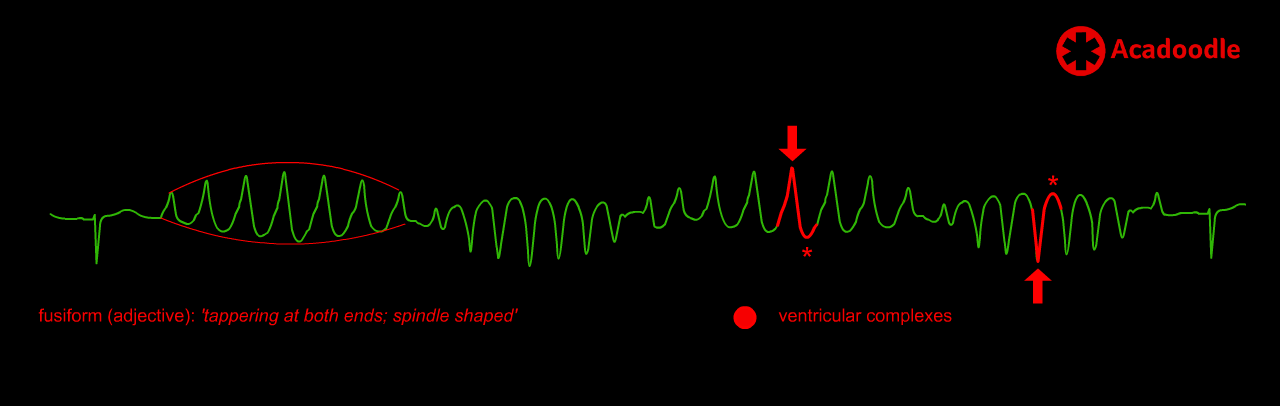
Groups of ventricular complexes demonstrate a fusiform shape (outlined by the curved red lines in the image above). This appearance results from a progressive increase in the amplitude of ventricular deflections followed by a progressive fall in their amplitude. Also, in this particular case, there is a clear asymmetry in the shape of the individual ventricular complexes. Each has a sharp point of maximal amplitude (arrow) and a curved component (red asterix). This makes identification of the cardinal characteristic of torsade de pointes straightforward; periodic reversal of the axis of ventricular depolarization.
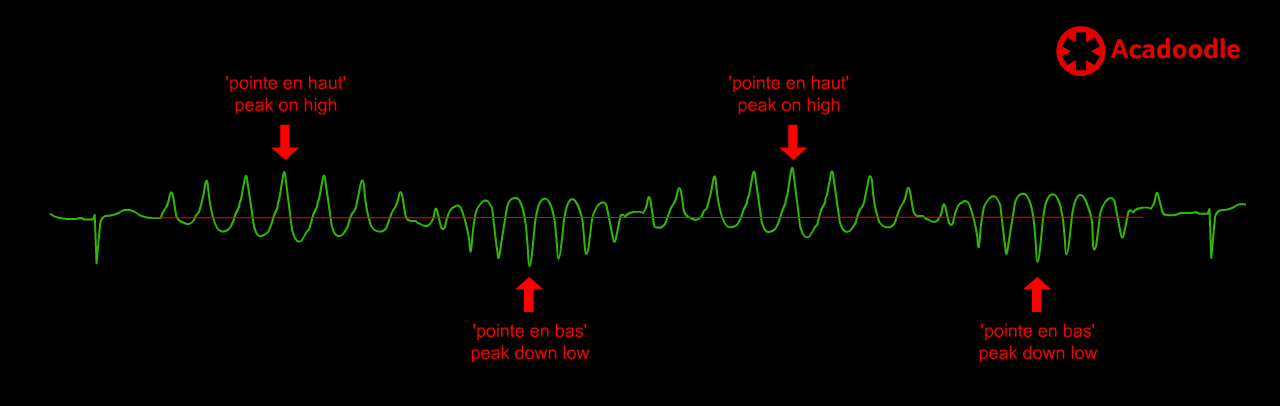
During the tachycardia, in the first fusiform group of ventricular complexes, the point of maximal amplitude (peak) of these deflections (arrow) is positive (above the isoelectric line). In the second group the point of maximal amplitude is negative (below the isoelectric line). This sequence is then repeated in the subsequent groups. The axes (direction of movement) of ventricular depolarization and repolarization events are rotating (twisting) around the isoelectric line (red line above). As in the case illustrated here, the polymorphic VT of torsade usually occurs in self-limiting paroxysms. This allows us identify the coexistence of QT prolongation on the ECG, a requirement to make this diagnosis.

The pathogenic mechanism underlying torsade de pointes is poorly understood. It is possible, as suggested in the original description of the arrhythmia, that during the tachycardia, rapid ventricular depolarization originates from two different sources situated at different anatomical sites within the ventricles, discharging depolarization for alternating periods of time (‘deux foyers opposés variables’). As the anatomical origin of depolarsization varies, the pattern of spread (axis) of ventricular depolarization and repolarization is expected to change as control of ventricular depolarization alternates between the sources. An intuitively more appealing hypothesis has been advanced in which the mechanism generating rapid ventricular depolarization, whatever its nature, itself, may periodically change anatomical location within the ventricles during the course of the tachycardia.
For exam purposes we can make some general points about management. When faced with torsade we 1) identify and hold any drugs capable of prolonging the QT interval and 2) correct electrolyte abnormalities (hypokalemia, hypomagnesemia). 3) Intravenous magnesium administration forms the mainstay of treatment for torsade de pointes. That’s all fine and reasonable, however, in real life, whenever you are faced with an irregular broad complex tachycardia, provided the patient is stable, the key point in management is to seek expert help. In torsade, degeneration into ventricular fibrillation and death may be precipitated by inappropriate treatment, including administration of certain anti-arrhythmic agents.
Pointe of interest: At medical school in Cambridge in the 1980s, we were told that the term ‘torsade de pointes’ referred to a spinning dance movement performed by a ballerina. I believed this to be true for many years and hearing the term always takes me to a better place. However, consulting the original paper which coined the phrase, I could find no mention of ballet. As is so often the case, much may have been gained in mistranslation!

1. Dessertenne, F. (1966). “La tachycardie ventriculaire à deux foyers opposés variables”. Archives des maladies du coeur et des vaisseaux. 59 (2): 263–272. ISSN 0003-9683. PMID 4956181.
DisclaimerPrivacy PolicyTerms of UseData Deletion© Acadoodle 2026